Understanding Healing, Wellness and Growth Pathways
Many Goals. Many Pathways. One Interconnected Human Journey.
Contents
Overview
Definitions and conceptual scope
Health as more than the absence of disease
Human flourishing as an organizing framework
Whole person health and systems thinking
Individual differences and personalized pathways
Physical health foundations
Brain plasticity, learning and adaptation
Mental and emotional well-being
Trauma recovery and restoration of safety
Relationships, belonging and community
Nature, environment and place
Meaning, purpose and existential growth
Positive psychology, character and personal development
Mindfulness, meditation and contemplative practice
Breathwork, somatic and body-based approaches
Integrative medicine and patient-centered care
Lifestyle medicine and behavior change
Education, coaching and learning pathways
Retreats, immersive experiences and transformational settings
Psychedelic-assisted and psychedelic-adjacent pathways
Spirituality, transcendence and belief change
Goals and pathway matching
Ethics, safety and responsible guidance
Research limits and future directions
Practical evaluation of providers and pathways
Conclusion
Understanding Healing, Wellness and Growth Pathways is a foundational overview of the routes through which people pursue relief from suffering, improved well-being, personal development, and human flourishing. It treats healing, wellness, and growth as overlapping dimensions of one interconnected human journey.
Research across public health, medicine, psychology, neuroscience, social science, environmental health, integrative medicine, and systems science supports a broad view of human well-being. People are biological, psychological, social, cultural, and meaning-making beings, not isolated symptoms or goals [1].
This article is written as an encyclopedia-style guide for readers seeking a clear, evidence-based map of the major pathways. It does not present any one tradition, practice, retreat, therapist, coach, medicine, or worldview as the answer to human suffering. Instead, it examines how many pathways can be understood within a professional, research-informed framework. Its central premise is simple: human beings are complex living systems, and meaningful healing and growth usually require attention to more than one dimension of life [2].
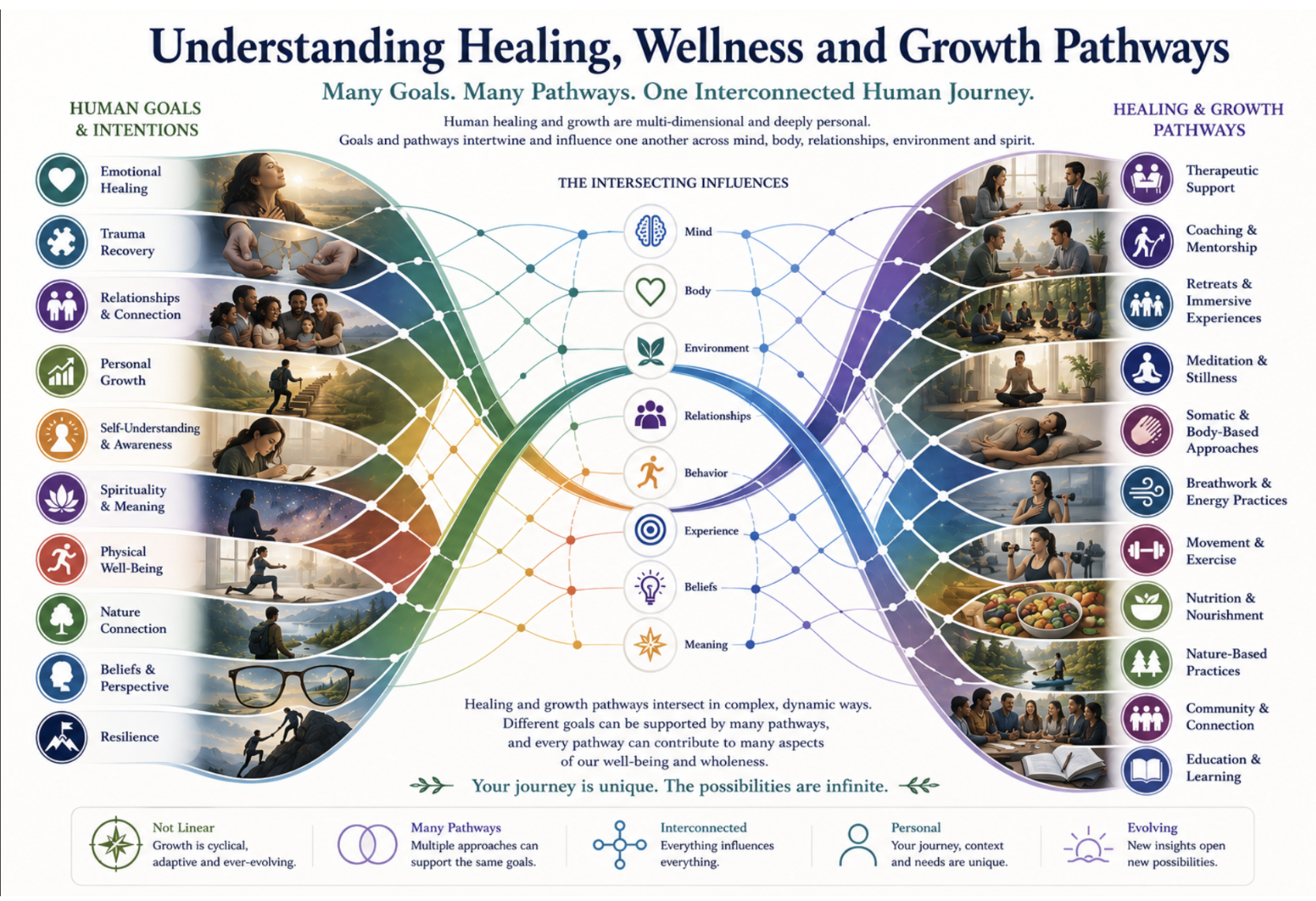
Figure 1. Understanding Healing, Wellness and Growth Pathways.
Overview
The language of healing, wellness, growth, and flourishing is used widely, but often imprecisely. Healing usually refers to recovery from injury, distress, illness, disconnection, or loss of function. Wellness usually refers to the active cultivation of health, balance, vitality, and supportive habits. Growth refers to learning, maturation, resilience, transformation, identity development, and expanded capacity. Flourishing refers to a broader condition in which multiple areas of life are going well, including physical and mental health, happiness and life satisfaction, meaning and purpose, character and virtue, close social relationships, and long-term stability [3].
These concepts overlap. A person recovering from depression may need clinical care, social support, exercise, improved sleep, spiritual meaning, and a more supportive environment. A person seeking personal growth may begin with coaching or education but discover unresolved trauma or relationship patterns. A person seeking spiritual meaning may also need physical health foundations, psychological support, and community. A person seeking trauma recovery may benefit from psychotherapy, body-based practices, safe relationships, mindfulness, and lifestyle changes. The point is not that everyone needs everything. The point is that human goals are interconnected.
The structure of this article follows that logic. It begins with the broad public health and whole person health foundations, then moves through physical health, mental health, relationships, environment, meaning, contemplative practice, integrative approaches, and transformational pathways. Later sections address complexity, individual differences, ethics, and practical application. This order is intentional. It places the most universal and foundational domains first, while treating more specialized and emerging interventions, including psychedelic-assisted therapies, as one area within a larger evidence ecosystem [4].
For a learning center, this approach is essential. Readers arrive through many doorways: therapy, coaching, retreats, meditation, breathwork, products, courses, legal questions, or general curiosity. A coherent Atlas helps connect those entry points without pretending they are the same.
Definitions and conceptual scope
Healing often describes repair, recovery, or restoration. In clinical settings it may refer to symptom reduction, wound healing, functional improvement, or recovery from illness. In personal and spiritual contexts, it may refer to becoming less dominated by pain, fear, grief, shame, or disconnection.
Wellness is often more proactive. It describes habits, environments, and practices that support health before crisis emerges. The Ottawa Charter for Health Promotion framed health promotion as enabling people to increase control over and improve their health, with attention to supportive environments, community action, personal skills, public policy, and health services [5]. This is important because wellness is not only an individual lifestyle project. It also depends on social determinants such as income, education, housing, safety, discrimination, community conditions, work, food access, and health care systems [6].
Growth refers to development over time. Growth may involve new skills, emotional maturity, insight, resilience, education, character development, or spiritual deepening. Neuroscience supports the general possibility of growth through plasticity, because the nervous system can change in response to learning, practice, and experience [7]. Psychology supports the possibility of growth through evidence-based methods that alter thought patterns, behavioral repertoires, coping strategies, values-based action, and relationships [8]. Social science supports the importance of growth through education, work, family, community, and institutions [9].
Pathways are routes, not guarantees. A pathway may be evidence-based for a specific condition, promising but still under study, supportive for some people, cultural or spiritual in nature, or inappropriate for a particular person. Precision matters.
Health as more than the absence of disease
A major shift in modern health thinking is the recognition that health is more than the absence of diagnosable disease. The World Health Organization has long defined health in broad physical, mental, and social terms, and its mental health materials emphasize well-being, coping, functioning, and community participation rather than merely the absence of mental disorder [10]. This broader view is central to an article about healing and growth because many people seeking help are not only asking how to remove symptoms. They are asking how to live better.
The social determinants of health literature makes clear that health is shaped by the conditions in which people are born, grow, live, work, and age [11]. These conditions influence exposure to stressors, access to resources, opportunities for education, health behaviors, social support, environmental hazards, and medical care. A person may be told to exercise, meditate, or eat better, but these recommendations have different meanings depending on safety, work schedule, income, disability, food access, caregiving burdens, and neighborhood design. Professional health education must avoid reducing all outcomes to individual willpower.
The biopsychosocial model also challenged the narrow biomedical focus on disease mechanisms alone. It argued that biological, psychological, and social dimensions interact in illness and care [12]. In practice, this means that chronic pain, depression, metabolic disease, trauma symptoms, sleep problems, substance misuse, anxiety, and many other issues cannot always be fully understood by looking only at tissue, neurotransmitters, or laboratory values. A person's beliefs, relationships, stress exposure, social role, behavior, and environment can influence both suffering and recovery.
Biology still matters. The point is that biology is embedded in life. Stress, sleep, food, movement, relationships, environment, and meaning can all influence how people function and recover.
Human flourishing as an organizing framework
Human flourishing provides one of the most useful organizing frameworks for healing, wellness, and growth. Tyler VanderWeele proposed that flourishing should be understood broadly, not only as happiness or life satisfaction, but as doing or being well across several domains of human life. These domains include happiness and life satisfaction, mental and physical health, meaning and purpose, character and virtue, and close social relationships. Financial and material stability may also be considered important for sustaining flourishing over time [13].
This model matters because it prevents a common mistake: treating one domain as if it were the whole of well-being. Happiness matters, but a person can feel pleasure while lacking purpose. Physical health matters, but physical fitness alone does not guarantee meaningful relationships. Mental health matters, but symptom reduction is not identical to flourishing. Spiritual experiences may be powerful, but they do not replace sleep, nutrition, ethical conduct, or social responsibility. A flourishing framework keeps the whole person in view.
Other influential psychological frameworks reinforce this wider view. Ryff's model of psychological well-being emphasizes self-acceptance, positive relations with others, autonomy, environmental mastery, purpose in life, and personal growth [14]. Self-determination theory emphasizes autonomy, competence, and relatedness as basic psychological needs that support motivation and well-being [15]. Positive psychology highlights meaning, engagement, relationships, accomplishment, positive emotion, and character strengths [16]. Meaning research shows that purpose, coherence, and significance can influence how people experience their lives [17].

Figure 2. Interconnected Dimensions of Well-Being.
Together, these frameworks suggest that healing and growth are not only about reducing distress. They are also about restoring agency, strengthening relationships, cultivating skills, building meaning, and participating more fully in life. For a lay reader, this may be the central insight: wellness is not one practice. It is the condition of many life-supporting systems becoming more coherent.
Whole person health and systems thinking
Whole person health is a research and care framework that emphasizes the interconnectedness of biological, behavioral, social, and environmental factors across individuals, families, communities, and populations. NCCIH's strategic plan placed whole person health at the center of its research agenda, describing the need to understand how different systems interact and how multicomponent interventions may affect multisystem outcomes [18].
The whole person perspective is especially important because modern medicine often organizes knowledge by organ system, disease category, or specialty. This structure is useful for diagnosis and treatment, but it can also create silos. Sleep influences mental health, immune function, metabolism, and pain. Stress influences inflammation, behavior, cardiovascular function, and relationships. Diet influences metabolism, cognition, inflammation, and mood. Movement influences musculoskeletal function, cardiovascular health, cognition, emotional regulation, and social participation. A whole person framework asks how these systems interact rather than treating them as unrelated topics [19].
Complexity science provides language for this problem. Health care and human behavior often function as complex adaptive systems. In such systems, many agents interact, outcomes are not always predictable, small changes may have large effects, and patterns emerge from relationships among parts [20]. This is different from a simple machine model in which every input produces a predictable output. A complex systems view helps explain why one person may respond strongly to a lifestyle change while another needs psychotherapy, medication, social support, or environmental change.
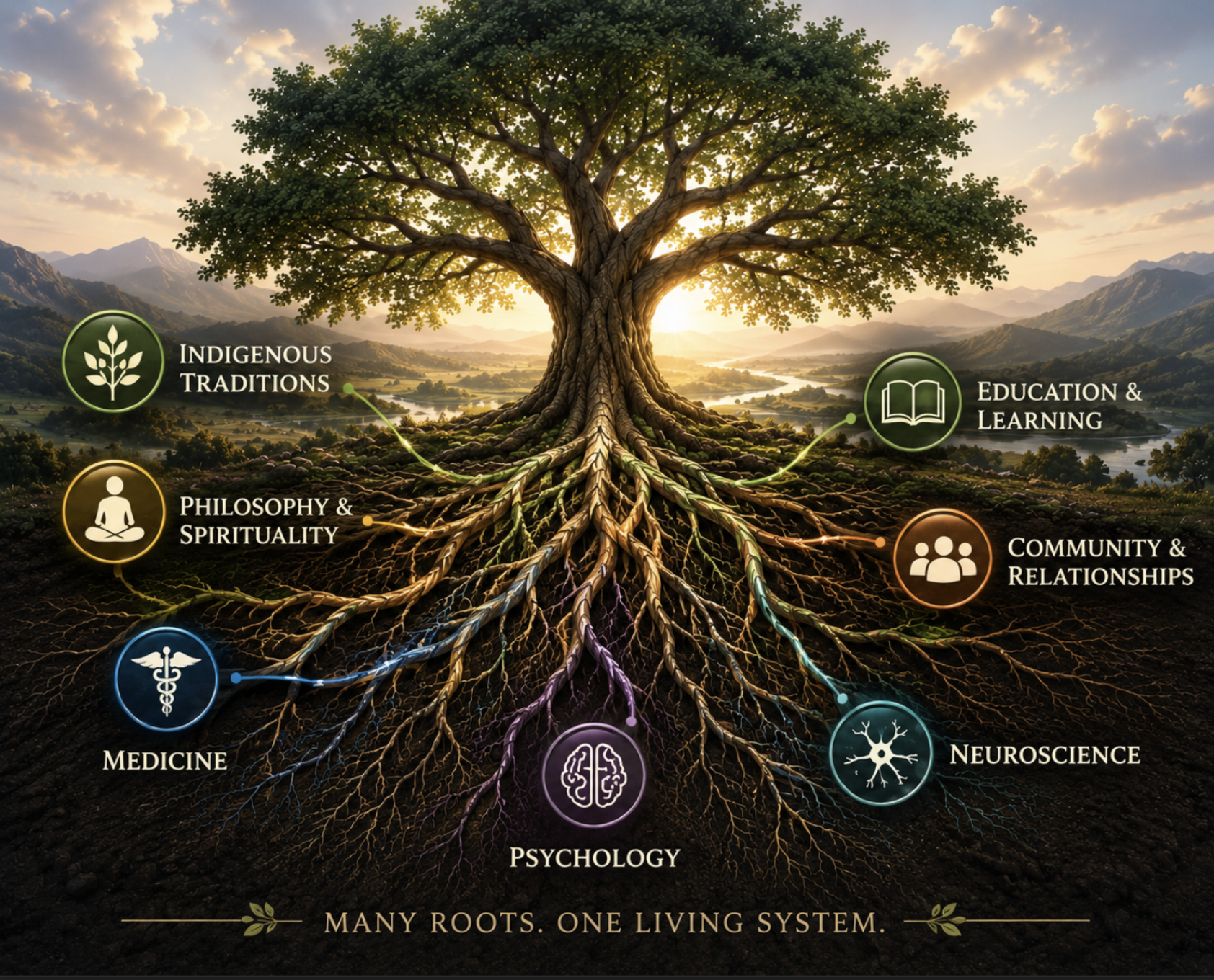
Figure 3. Many Roots. One Living System.
The practical implication is that healing pathways should be integrated without being confused. Integration does not mean treating every approach as equally valid or equally supported. It means understanding how different evidence-based and promising approaches may interact within the life of a particular person. The best systems framework is both open and disciplined. It is open enough to include body, mind, relationships, environment, culture, and meaning. It is disciplined enough to ask about evidence, safety, mechanism, context, and outcomes.
Individual differences and personalized pathways
People differ in biology, history, culture, goals, resources, risks, and responsiveness to interventions. For that reason, a serious pathway framework cannot assume that one approach will work equally well for everyone. Precision medicine, personalized evidence-based medicine, and research on heterogeneous treatment effects all point toward the importance of matching interventions to individuals and contexts [21].
Heterogeneous treatment effects occur when an intervention helps some people more than others, helps different people in different ways, or carries different risks for different groups [22]. This concept is essential for mental health, lifestyle change, integrative medicine, and growth practices. A treatment may be highly beneficial on average but less appropriate for a specific person because of medical history, trauma history, medication use, personality, cultural context, financial constraints, or preference. Conversely, an intervention that appears modest on average may be very helpful for a subgroup.
Personalized pathways do not mean abandoning evidence. They mean using evidence more intelligently. Research can identify likely benefits, known risks, mechanisms, and typical outcomes. Practitioners and individuals can then consider personal goals, values, readiness, support systems, and constraints. The question is not merely, 'Does this work?' It is, 'For whom, under what conditions, for which goal, with what risks, and compared with what alternative?'
This point is especially important for a marketplace or learning center that includes many categories of providers and practices. A reader seeking trauma recovery may need a licensed trauma therapist before a retreat. A reader seeking better energy may need medical evaluation, sleep improvement, and nutrition before advanced breathwork. A reader seeking spiritual growth may need grounding and community support. A reader with severe depression or suicidal thoughts needs clinical assessment, not general wellness advice. Matching goals to pathways is a professional responsibility.
Physical health foundations
Physical health is one of the strongest foundations for healing and growth because the body provides the biological platform through which cognition, emotion, energy, social participation, and behavior occur. The evidence base for physical activity, nutrition, sleep, and chronic disease prevention is extensive and far stronger than the evidence for many specialized wellness practices [23].
Physical activity is associated with reduced risk of many chronic diseases, improved cardiovascular and metabolic health, better functional capacity, and improved mental health outcomes [24]. Exercise is not only a fitness practice. It is a broad health intervention. Aerobic activity, resistance training, balance training, mobility work, and everyday movement all support different aspects of health. Movement can also influence confidence, agency, mood, sleep, and social connection when practiced in supportive environments.
Sleep is another foundational pathway. Consensus recommendations for adult sleep emphasize the importance of adequate sleep duration for health, performance, safety, and well-being [25]. Poor sleep can worsen mood, pain sensitivity, attention, immune function, appetite regulation, and stress tolerance. Because sleep influences so many systems, sleep improvement can sometimes produce cascading benefits across mental health, energy, behavior, and relationships.
Nutrition provides the biological inputs required for maintenance, repair, immunity, metabolism, and brain function. The Dietary Guidelines scientific report and major nutrition reviews emphasize dietary patterns rather than single miracle foods [26]. A prudent nutrition framework focuses on adequate nutrient intake, dietary quality, reduced excess of harmful patterns, and long-term sustainability. For most people, the central question is not which extreme diet is fashionable, but which dietary pattern supports health, energy, metabolic function, and adherence over time.
Chronic disease prevention research shows that many of the most serious health burdens are influenced by modifiable risk factors, social conditions, and public policy [27]. This does not mean every disease is preventable or every person is responsible for illness. It means that environments, behaviors, resources, and systems can shift population risk. For an individual reader, physical health foundations are often the most practical starting point. For a public health system, they are among the most important long-term investments.
Brain plasticity, learning and adaptation
Brain plasticity is the capacity of the nervous system to change in response to experience, learning, behavior, and injury. It is one reason human beings can develop new skills, recover function, form new habits, revise beliefs, adapt to changing circumstances, and benefit from psychological or behavioral interventions [28].
Plasticity does not mean the brain can be reshaped instantly or without limits. It means that the nervous system is dynamic. Repetition, attention, emotional salience, environment, physical activity, relationships, and learning conditions can influence neural pathways. This is relevant to healing because many patterns of distress, avoidance, attention, emotion, and behavior are learned over time. It is relevant to growth because new patterns can also be cultivated over time.
Psychotherapy, mindfulness practice, exercise, education, social experience, and contemplative disciplines can all be understood partly through adaptation and learning. The mechanisms differ. Cognitive behavioral therapy may alter appraisals and behaviors. Acceptance and commitment therapy may alter relationships to thoughts and feelings. Exercise may affect neurotrophic factors, vascular health, sleep, mood, and cognition. Meditation may train attention and awareness. Social safety may reduce threat responses and improve emotion regulation. These are not identical pathways, but all involve experience-dependent change [29].
The concept of plasticity also invites caution. Human systems can adapt in harmful directions. Chronic stress, trauma, isolation, sedentary behavior, poor sleep, substance misuse, and repeated avoidance can reinforce patterns that undermine well-being. Growth therefore requires not only adding positive practices but also changing the conditions that maintain harmful adaptation. In this sense, healing is often ecological: it depends on the repeated environments, relationships, practices, and interpretations that shape a person over time.
Mental and emotional well-being
Mental and emotional well-being includes emotional regulation, cognitive flexibility, resilience, coping capacity, self-understanding, motivation, and the ability to function in relationships and daily life. It is not limited to the absence of a psychiatric diagnosis. A person may not meet criteria for a disorder and still feel disconnected, chronically stressed, purposeless, emotionally dysregulated, or unable to pursue valued goals [30].
Cognitive behavioral therapy has one of the strongest evidence bases in psychotherapy. Reviews of meta-analyses show its efficacy across a wide range of conditions, including anxiety disorders, depression, and other psychological problems [31]. CBT is built on the relationship between thoughts, emotions, behaviors, and physiological responses. It helps people identify unhelpful patterns, test beliefs, change behaviors, and build skills. Its importance in a broad pathway article is not that it replaces all other approaches, but that it provides a rigorous model of how structured psychological intervention can reduce suffering.
Acceptance and commitment therapy offers a complementary model. ACT emphasizes psychological flexibility, values-based action, acceptance, defusion from thoughts, contact with the present moment, self-as-context, and committed action [32]. Psychological flexibility has been described as a fundamental aspect of health because it supports adaptation across changing conditions [33]. In plain language, it helps people stop organizing life only around avoidance of pain and start organizing life around meaningful action.
Resilience research adds another layer. Resilience is not a fixed trait possessed by a heroic few. It is a dynamic process shaped by biology, development, relationships, culture, meaning, coping strategies, and social resources [34]. People may be resilient in one domain and vulnerable in another. Communities and institutions can also be more or less resilient. A professional article should avoid simplistic slogans such as 'be resilient' and instead explain that resilience is built through support, skills, adaptation, and conditions that make recovery possible.
Mental and emotional well-being therefore includes both clinical and developmental pathways. Clinical pathways help reduce symptoms and treat disorders. Developmental pathways build self-awareness, flexibility, values, emotional capacity, and meaning. A complete learning center should respect both without confusing them. A coach, retreat, meditation teacher, or wellness provider may support growth, but serious mental health conditions often require licensed clinical care.
Trauma recovery and restoration of safety
Trauma can affect the body, mind, relationships, identity, and sense of safety. It may arise from acute events, repeated exposure, relational harm, violence, neglect, medical experiences, social oppression, disaster, or chronic threat. Trauma recovery is therefore rarely only intellectual. People may need to restore safety in the nervous system, body, relationships, environment, and meaning structure.
The sources assembled for this article do not reduce trauma recovery to one method. They support a multi-pathway view. Evidence-based psychotherapies can help people process thoughts, emotions, memories, and avoidance patterns [35]. Psychological flexibility can help people relate differently to painful internal experiences [36]. Social relationships and community support can reduce isolation and strengthen recovery [37]. Body-oriented therapies, slow breathing, and related practices may support regulation for some individuals, though evidence strength varies by modality [38].
Safety is a central concept. A person cannot always think, reflect, or grow effectively when the body and nervous system are organized around threat. Supportive relationships, stable environments, predictable routines, sleep, movement, and professional care can all contribute to a greater sense of safety. This does not mean comfort at all times. Growth often involves difficulty. But difficulty is more likely to become growth when it occurs inside an adequate container of support, consent, pacing, and integration.
Trauma recovery also requires ethical caution. Intensive retreats, breathwork, psychedelic sessions, somatic practices, and spiritual experiences can be meaningful for some people, but they can also overwhelm people with trauma histories if poorly facilitated. A professional pathway framework should ask whether a provider is trained, whether screening occurs, whether consent is clear, whether follow-up support exists, whether medical or psychiatric risks are considered, and whether the practice is appropriate for the individual's condition.
The goal of trauma recovery is not simply to erase the past. It is often to reduce the past's domination of the present, restore agency, increase connection, improve regulation, and support meaningful participation in life. That goal may require multiple pathways, and the sequence matters. For some people, stabilization comes before deep exploration. For others, relationship repair, body regulation, or purpose may become the doorway into recovery.
Relationships, belonging and community
Social connection is one of the most powerful and consistent themes in the evidence base for well-being. Meta-analytic research has found that social relationships are associated with mortality risk, and later work has identified loneliness and social isolation as risk factors for health [39]. These findings matter because they place relationships in the same serious conversation as physical health behaviors. Connection is not a luxury. It is a health-relevant condition.
The World Health Organization's work on social determinants of mental health emphasizes that mental health is shaped by social, economic, and environmental conditions [40]. Poverty, discrimination, exclusion, violence, unemployment, poor housing, and weak social support can all affect mental health. A person seeking healing may need therapy, but they may also need safety, housing, belonging, purpose, and community. Without this wider view, wellness culture can become unfairly individualistic.
Social baseline theory offers a useful psychological perspective. It suggests that humans are adapted to regulate emotion and respond to the world with others, not as isolated individuals [41]. Social proximity and support can reduce perceived threat and the effort required to face challenges. This helps explain why secure relationships, mentoring, peer support, family repair, and community belonging can change how people experience stress and possibility.
Community well-being research extends this from individual relationships to shared life. Communities can support or undermine flourishing through trust, participation, shared resources, safety, culture, institutions, and collective identity [42]. A person may develop through individual effort, but that effort is shaped by communities. The healthiest pathway ecosystem does not simply connect individuals to services. It also helps people find belonging, accountability, contribution, and shared meaning.
This is why relationship and community pathways should appear near the center of any framework for healing and growth. Therapy can help repair relational wounds. Coaching can support communication and leadership. Retreats can create temporary communities of practice. Meditation groups, movement communities, nature groups, and educational programs can reduce isolation. But the quality of relationship matters. Connection supports healing when it is safe, respectful, ethical, reciprocal, and grounded.
Nature, environment and place
Human well-being is shaped by place. Environmental health research shows that neighborhoods, green space, housing, air quality, transportation, safety, built environments, and access to resources influence health and behavior [43]. Nature-based and environmental pathways should therefore be understood at both personal and public levels. A walk in a forest may support restoration for an individual. Equitable access to parks, clean air, safe streets, and healthy housing supports population well-being.
A systematic review and meta-analysis of greenspace exposure found associations between contact with green environments and multiple health outcomes [44]. Nature connectedness research also suggests a relationship between feeling connected to nature and happiness [45]. Environmental psychology has long studied the restorative benefits of nature, including attention restoration, stress reduction, and recovery from mental fatigue [46]. Earlier work on aesthetic and affective responses to natural environments helped establish that landscape and environment can influence emotional experience [47].
These findings support a practical conclusion: nature connection is not merely recreational. It can be a pathway into regulation, perspective, awe, embodiment, and belonging. For some people, nature-based practices may reduce rumination, support movement, restore attention, and create a felt sense of connection beyond self-focused concerns. For others, access to nature may be limited by disability, location, climate, safety, time, or economic constraints. A responsible article should treat nature as valuable without romanticizing it as universally accessible or sufficient.
The biophilia hypothesis and related literature argue that humans may have deep affinities with living systems and natural environments [48]. Whether framed philosophically, psychologically, or biologically, this idea resonates with many people's experience that nature can support meaning and emotional restoration. At the same time, environmental pathways must remain grounded in evidence and public health reality. The built environment can promote or obstruct movement, social interaction, safety, and access to nutritious food [49].
For Psychedelist's learning center structure, nature-based practices can be understood as one pathway among many. They may intersect with meditation, movement, retreats, indigenous traditions, ecological spirituality, community, and education. The key is to place nature within an integrated framework rather than using it as a vague wellness symbol.
Meaning, purpose and existential growth
Meaning and purpose are central to many healing and growth journeys. People often seek help not only because they are anxious, depressed, grieving, or physically unwell, but because life feels directionless, fragmented, or disconnected from what matters. Meaning gives suffering context. Purpose gives behavior direction. Both can influence motivation, resilience, and long-term well-being [50].
Viktor Frankl's existential psychology and logotherapy placed meaning at the center of human life, especially in the face of suffering [51]. While not all modern researchers adopt Frankl's full philosophical framework, the enduring importance of his work lies in its insistence that people need more than comfort. They need a reason to live, values to serve, and a way to relate to suffering that does not reduce them to victims of circumstance.
Empirical research supports the relevance of purpose to health. Hill and Turiano found that purpose in life predicted mortality across adulthood [52]. VanderWeele's flourishing framework includes meaning and purpose as one of the central domains of human flourishing [53]. Steger's work on meaning in life and well-being helps clarify how meaning contributes to psychological health [54]. These sources support the view that meaning is not merely abstract philosophy. It is a measurable and consequential dimension of life.
Purpose can arise through many routes: family, vocation, service, creativity, education, spirituality, recovery, activism, mentorship, art, nature, or community. It can also change over time. A person's purpose at 20 may not be the same as at 50. Loss, illness, transition, aging, and spiritual experience can all reorganize priorities. A pathway framework should therefore leave room for evolving identity and meaning.
Existential growth often involves difficult questions. What matters? What kind of person am I becoming? What is worth suffering for? What relationships need repair? What responsibilities am I avoiding? What must be grieved? What can be forgiven? What can no longer be postponed? These questions are not answered by wellness tips alone. They require reflection, support, courage, and often community.
Positive psychology, character and personal development
Positive psychology emerged partly to study strengths, virtues, flourishing, and positive human functioning rather than focusing only on pathology. This does not mean ignoring suffering. It means asking what helps individuals and communities thrive. Seligman's PERMA framework emphasizes positive emotion, engagement, relationships, meaning, and accomplishment [55]. VanderWeele's framework similarly includes happiness, health, meaning, character, relationships, and stability [56].
Positive psychology intervention research suggests that some intentional activities can improve well-being, although effects vary by intervention, population, and study quality [57]. Such interventions may include gratitude practices, strengths exercises, acts of kindness, optimism practices, and meaning-oriented reflection. These tools are not substitutes for clinical treatment when clinical treatment is needed, but they can support growth and well-being in appropriate contexts.
Character strengths research by Park, Peterson, and Seligman linked strengths of character with well-being [58]. This is important because it widens the conversation beyond feeling good. Flourishing also involves becoming capable of honesty, courage, kindness, self-regulation, wisdom, gratitude, perseverance, and contribution. A person may improve mood without improving character, and a society may increase pleasure without increasing responsibility. A serious flourishing article should include virtue without moralizing.
Flow research adds another dimension. Csikszentmihalyi's work on flow describes states of deep absorption in activities that balance challenge and skill [59]. Flow can occur in art, sport, work, learning, spiritual practice, and skilled service. It suggests that growth is not only reflective. It is also participatory. People develop through doing difficult, meaningful things with attention and increasing skill.
Personal development therefore includes more than self-improvement branding. It includes the cultivation of capacities: attention, discipline, emotional regulation, honesty, courage, learning, relational skill, and service. Coaching, mentorship, education, therapy, spiritual practice, and community can all contribute when they are ethically grounded and matched to the person's goals.
Mindfulness, meditation and contemplative practice
Mindfulness and meditation occupy a major place in contemporary wellness culture, but their responsible presentation requires precision. Mindfulness-based stress reduction has been studied in relation to stress and health benefits, with meta-analytic evidence suggesting potential value across several outcomes [60]. Meditation programs have also been examined in systematic reviews and meta-analyses for psychological stress and well-being [61].
Meditation is not one thing. Practices differ in attentional focus, open monitoring, compassion, mantra, movement, breath awareness, visualization, prayer, and philosophical context. Some are secularized clinical interventions. Others are embedded in religious or spiritual traditions. Because practices differ, claims should be specific. It is more accurate to say that certain meditation programs have evidence for certain outcomes than to say meditation works for everything.
The most credible role for mindfulness in a healing and growth framework is as a self-regulation and awareness pathway. Mindfulness can help people notice thoughts, emotions, sensations, impulses, and habitual reactions. It can create space between stimulus and response. It can support acceptance, compassion, attention, and values-based action. It may also help people become less fused with thoughts and less reactive to discomfort, overlapping conceptually with psychological flexibility [62].
Meditation also has limits and risks. Some people experience distress, dissociation, trauma activation, or destabilization during intensive practice. People with severe psychiatric symptoms or trauma histories may need adapted practices and professional support. A professional article should avoid implying that meditation is universally benign or always appropriate. Like any pathway, it requires context, skill, and fit.
Contemplative practice can also support meaning and spiritual growth. It may help people encounter silence, mortality, compassion, forgiveness, awe, or a sense of connection. But those dimensions should not be collapsed into clinical outcomes alone. A well-rounded framework can recognize both the mental health evidence and the deeper human questions that lead many people to contemplative paths.
Breathwork, somatic and body-based approaches
Breathwork, somatic practices, and body-based approaches are increasingly popular in wellness, trauma recovery, and personal growth settings. The evidence base varies widely by practice, population, and outcome. Some practices have stronger physiological rationale and empirical support than others. For that reason, this domain should be presented carefully, neither dismissed wholesale nor exaggerated.
Slow breathing research suggests that breathing patterns can influence autonomic function and cardiovascular regulation. Reviews have examined physiological effects of slow breathing, and specific studies have found effects on baroreflex sensitivity and blood pressure in essential hypertension [63]. In practical terms, breathing is one route through which voluntary behavior may influence arousal, attention, and bodily state. This makes breath regulation a plausible support for stress management, emotional regulation, and body awareness.
Somatic and body-oriented psychotherapy research has examined approaches that incorporate posture, movement, bodily sensation, expression, and embodied awareness into psychological work [64]. These approaches may be especially relevant for people whose distress is experienced strongly through the body. However, the field is diverse, and not all body-based practices have the same evidence base. Claims should be tied to specific methods and outcomes.
Polyvagal theory has influenced trauma and somatic practice communities by emphasizing autonomic regulation, social engagement, and physiological states related to safety and threat [65]. It has been influential as a conceptual model, but it should be used carefully and not treated as settled proof for every clinical claim made in its name. The more defensible point is that autonomic regulation, social safety, and body state are relevant to emotional experience and therapeutic work.
Breathwork and somatic approaches also raise safety questions. Intensive breathing can produce strong physical and emotional effects, and may be inappropriate for some medical or psychiatric conditions. Body-based work also requires clear consent, professional boundaries, trauma sensitivity, and appropriate training. These methods can be valuable pathways, but they must be presented within an ethical and evidence-aware framework.
Integrative medicine and patient-centered care
Integrative medicine developed partly in response to patient interest in complementary practices and partly in response to recognition that conventional care often does not address the whole person. The Institute of Medicine's summit on integrative medicine and the health of the public emphasized prevention, patient-centered care, lifestyle, therapeutic relationships, and the need to evaluate complementary approaches responsibly [66]. Maizes, Rakel, and Niemiec argued for integrative medicine as patient-centered care that considers the full range of physical, emotional, mental, social, spiritual, and environmental influences [67].
Patient-centered care is central to this discussion. Epstein and Street described the values and value of patient-centered care, emphasizing that care should respond to patients as persons, not merely disease carriers [68]. Mead and Bower's conceptual framework reviewed patient-centeredness in terms of biopsychosocial perspective, patient-as-person, shared power and responsibility, therapeutic alliance, and doctor-as-person [69]. These ideas align strongly with the broader goal of healing and growth pathways.
Integrative medicine does not mean uncritical acceptance of all alternative practices. Jonas and colleagues described the evolution of complementary and alternative medicine in the United States and the movement toward integration, while also discussing evidence, policy, research methods, and whole systems questions [70]. A mature integrative framework must be evidence-informed, safety-conscious, and transparent about uncertainty. It should ask whether a practice is effective, for whom, at what cost, with what risks, and in what relationship to conventional care.
Acupuncture provides an example of a complementary practice with a substantial research literature. An individual patient data meta-analysis found acupuncture to be associated with benefits for chronic pain compared with controls, though interpretation depends on condition, comparator, and clinical context [71]. This does not make acupuncture a universal solution. It does show how integrative practices can be evaluated using rigorous methods and placed appropriately within care options.
The best version of integrative care is not a marketplace of disconnected services. It is a coordinated approach that respects evidence, clinical responsibility, patient goals, prevention, lifestyle, and the complexity of human life. For readers, the practical lesson is to seek providers who can explain scope, evidence, risks, and fit without making exaggerated promises.
Lifestyle medicine and behavior change
Lifestyle medicine focuses on health behaviors and daily conditions that influence chronic disease risk and overall well-being. Nutrition, exercise, sleep, stress management, avoidance of harmful substances, and social connection are not minor add-ons. They are among the most powerful determinants of long-term health [72].
Dietary research supports the importance of overall dietary patterns rather than isolated nutrients or miracle foods. Katz and Meller argued that although many diet debates persist, common themes of healthful eating patterns are identifiable, including minimally processed foods, plants, and dietary quality [73]. The Dietary Guidelines scientific report similarly emphasizes evidence-based dietary patterns across the lifespan [74]. Nutrition should be personalized enough to account for culture, medical needs, and preference, but rigorous enough to avoid unsupported claims.
Exercise as medicine has been reviewed across many chronic diseases, with evidence supporting prescribed physical activity as therapy for numerous conditions [75]. Movement supports cardiovascular health, metabolic function, musculoskeletal health, mood, cognition, and function. For many people, the most sustainable exercise pathway is not extreme performance, but consistent movement matched to capacity, health status, and enjoyment.
Behavior change is difficult because habits are embedded in stress, identity, environment, time, relationships, access, and reward systems. Telling people what to do is rarely enough. Effective behavior change often requires skill building, supportive environments, accountability, feedback, meaning, and realistic planning. This is where coaching, education, community programs, and therapeutic support may play constructive roles when they stay within scope and use evidence-informed methods.
Lifestyle medicine also illustrates why individual and public health perspectives must be combined. A person can improve diet and exercise, but social determinants influence what is possible. Work schedules, income, neighborhood safety, food access, family obligations, disability, and health literacy all matter [76]. A professional wellness article should encourage agency while acknowledging structural reality.
Education, coaching and learning pathways
Education is one of the major pathways to flourishing identified in VanderWeele's review of determinants of human flourishing [77]. Education can improve knowledge, opportunity, agency, income, health literacy, civic participation, and personal development. In the context of healing and growth, education should be understood broadly: formal schooling, therapeutic education, health education, spiritual education, mentorship, coaching, skill training, and reflective learning all shape how people understand and act in their lives.
Coaching and mentorship occupy a different role from clinical therapy. Coaching may support goals, habits, accountability, identity development, leadership, relationships, lifestyle change, and performance. Mentorship may transmit wisdom, social support, professional development, and moral formation. These pathways can be valuable, but they require clarity of scope. Coaches should not diagnose or treat mental disorders unless they are also licensed and qualified to do so. Ethical coaching recognizes when referral to clinical care is needed.
Learning pathways are especially important because many people do not know how different wellness options relate to one another. A person may search for a retreat when they need trauma therapy. Another may seek medication when lifestyle foundations are severely disrupted. Another may pursue spiritual practice while avoiding relationship repair. Education can help people map goals to pathways and make better decisions.
A high-quality learning center should therefore function as a bridge between public understanding and professional standards. It should translate research into accessible language, define terms, compare pathways, explain evidence levels, identify risks, and help readers ask better questions. It should not overwhelm readers with jargon, but it should also not dilute complex research into slogans. This balance is the core editorial challenge of the Psychedelist Learning Center model.
Education also supports agency. When people understand how sleep, stress, relationships, environment, meaning, trauma, and behavior interact, they are more likely to make informed choices. They can also become less vulnerable to exaggerated claims. In this sense, education is itself a healing and growth pathway.
Retreats, immersive experiences and transformational settings
Retreats and immersive experiences can create temporary environments for reflection, learning, community, spiritual practice, emotional processing, or behavioral reset. They may include meditation, yoga, nature immersion, coaching, group work, ritual, creative expression, therapeutic support, or psychedelic-assisted work where legal and medically appropriate. Their potential value lies partly in removing people from ordinary patterns and placing them in structured settings that support attention and change.
However, immersive settings also carry risks. Intensity can be mistaken for healing. Emotional breakthrough can be mistaken for integration. Group belonging can be mistaken for long-term support. A powerful experience can fade if it is not connected to daily life, relationships, habits, and continuing care. A professional article should therefore distinguish experience from transformation. Transformation requires integration over time.
The whole person and complex systems frameworks are useful here [78]. A retreat is not an isolated intervention. It interacts with the person's prior trauma history, expectations, physical health, social support, beliefs, and post-retreat environment. The same retreat may be restorative for one person and destabilizing for another. Screening, facilitation quality, consent, aftercare, medical considerations, and ethical leadership are therefore central.
Retreats may be most appropriate when they are presented as part of a broader pathway rather than a complete solution. A meditation retreat may deepen practice but should not replace urgent psychiatric care. A coaching retreat may clarify goals but should not treat severe trauma. A spiritual retreat may support meaning but should not pressure participants into belief. A psychedelic retreat may involve profound experiences but should not be marketed as a guaranteed cure.
For learning center architecture, retreats belong in the section of pathways that can support growth, meaning, community, nature connection, or therapeutic work, depending on design. The article should help readers evaluate retreats by asking about evidence, safety, facilitator credentials, screening, group size, integration, emergency procedures, and ethical transparency.
Psychedelic-assisted and psychedelic-adjacent pathways
Psychedelic-assisted pathways require careful placement in a professional article. They are important to the Psychedelist ecosystem, but they should not dominate the foundation. The evidence base for human flourishing begins with health, relationships, meaning, environment, behavior, and systems. Psychedelic science appears later as an emerging and specialized domain within mental health and transformational experience research [79].
Clinical research has found promising outcomes for selected psychedelic-assisted therapies under controlled conditions. A phase 3 trial of MDMA-assisted therapy for severe PTSD reported significant effects compared with placebo-assisted therapy in a structured clinical protocol [80]. Ketamine research, including a systematic review and individual participant data meta-analysis, has shown rapid reductions in suicidal ideation after a single intravenous dose in controlled studies, although questions remain about duration, maintenance, and long-term outcomes [81].
A meta-analysis of placebo-controlled trials of psychedelic-assisted therapy found substantial effects across selected studies, but the field remains limited by sample sizes, blinding challenges, expectancy effects, heterogeneity of interventions, and the need for more rigorous long-term data [82]. The most responsible interpretation is neither dismissal nor hype. Psychedelic-assisted therapy is a serious area of research with promising findings for some conditions, but it requires clinical standards, careful screening, trained support, legal compliance, and integration.
Neuroplasticity is one proposed mechanism of psychedelic effects. A systematic review on psychedelics and neuroplasticity examined preclinical and clinical evidence related to neurogenesis, synaptogenesis, dendritic growth, BDNF, and other biological mechanisms [83]. These mechanisms may help explain why psychedelic experiences can sometimes produce lasting changes in mood, perspective, or behavior. However, mechanistic plausibility is not the same as universal clinical efficacy. Context, preparation, support, dose, compound, diagnosis, expectations, and integration all matter.
Mystical-type experiences and ego dissolution are also discussed in the literature. They may be associated with personal meaning, spiritual significance, or altered self-experience [84][85]. These findings should be presented carefully because profound experiences do not automatically produce stable healing or ethical practice.
Psychedelic pathways also require ethical clarity. They are not appropriate for everyone. Risks may include psychological distress, destabilization, unsafe settings, exploitation, legal consequences, medication interactions, cardiovascular concerns, and worsening of certain psychiatric conditions. The safest and most defensible presentation is that psychedelic-assisted therapies are emerging clinical and experiential pathways that may be valuable for selected people in appropriate settings, but they do not replace foundational health, mental health care, relationships, ethics, or integration.
Spirituality, transcendence and belief change
Spirituality and transcendence appear across many healing and growth traditions. Some people understand healing through religion, prayer, ritual, indigenous traditions, meditation, nature, mystical experience, service, moral repair, or relationship with the sacred. Others use secular language of meaning, awe, values, consciousness, or connection. A professional article can acknowledge these experiences without reducing them to pathology or making unsupported metaphysical claims.
The source library includes multiple pathways into spirituality and transcendence. Frankl's meaning-centered work addresses the human need for purpose in suffering [86]. Mindfulness and contemplative research examines practices that may alter attention, stress, and self-relation [87]. Psychedelic research examines mystical-type experience, personal meaning, spiritual significance, and ego dissolution [88]. Positive psychology and flourishing frameworks include meaning, purpose, character, virtue, and relationships [89].
Beliefs and perspective can shape well-being. People interpret suffering through narratives. They may believe they are broken, punished, abandoned, unsafe, capable, supported, called, responsible, or connected. Some beliefs restrict growth. Others support resilience and action. Cognitive therapies address maladaptive beliefs directly [90]. ACT helps people relate differently to thoughts while acting according to values [91]. Spiritual traditions may help people place suffering within a larger moral or cosmic frame.
The challenge is to respect meaning without abandoning discernment. Not every spiritual claim is true, safe, or helpful. Not every intense experience is wisdom. Not every teacher is trustworthy. Spiritual communities can heal, but they can also harm. A learning center should encourage humility, ethical safeguards, informed consent, cultural respect, and attention to power dynamics.
Spiritual and transcendence pathways are therefore best understood as meaning-oriented pathways. They may help people encounter awe, humility, forgiveness, connection, mortality, gratitude, and purpose. Their value depends not only on the experience itself, but on how it shapes character, relationships, responsibility, and daily life.
Goals and pathway matching
Because people arrive with different goals, a professional framework should help match goals to pathways. Emotional healing may call for psychotherapy, mindfulness, supportive relationships, sleep restoration, and body regulation. Trauma recovery may require trauma-informed clinical care, stabilization, somatic support, careful pacing, and community. Relationship repair may involve therapy, communication training, family work, support groups, or mentorship. Physical well-being may require movement, nutrition, sleep, medical evaluation, and behavior change. Spirituality and meaning may involve contemplative practice, community, nature, study, service, or retreat settings.
Personal growth may be supported by coaching, education, mentorship, therapy, flow activities, values clarification, and character development. Self-understanding may involve psychotherapy, journaling, meditation, assessment, conversation, and reflection. Nature connection may be supported by outdoor practices, ecological education, movement in natural settings, and community. Beliefs and perspective may be addressed through CBT, ACT, philosophical reflection, spiritual practice, education, and meaningful experience. Resilience may be built through skills, relationships, physical health, meaning, and adaptive challenge [92].
The same pathway can serve multiple goals. Exercise may support physical vitality, mood, sleep, confidence, and social connection. Meditation may support attention, emotional regulation, spirituality, and self-understanding. Therapy may support trauma recovery, relationship repair, meaning, and behavior change. Community may support belonging, accountability, purpose, and resilience. Nature may support stress reduction, awe, movement, and perspective. This is why pathway systems should be represented as networks rather than simple ladders.
The reverse is also true: the same goal can be supported by multiple pathways. A person seeking emotional healing might benefit from therapy, movement, breath regulation, social support, meaning work, and nature. A person seeking purpose might benefit from education, service, spiritual practice, coaching, therapy, and community. The art of pathway selection lies in sequencing, fit, safety, and integration.
This framework supports a clear editorial standard for Psychedelist articles. Each article should define the goal, describe relevant pathways, summarize evidence, identify risks, explain who may benefit, and clarify when professional care is needed. That approach is stronger for SEO, stronger for Google Ads compliance, and stronger for reader trust than promotional language.
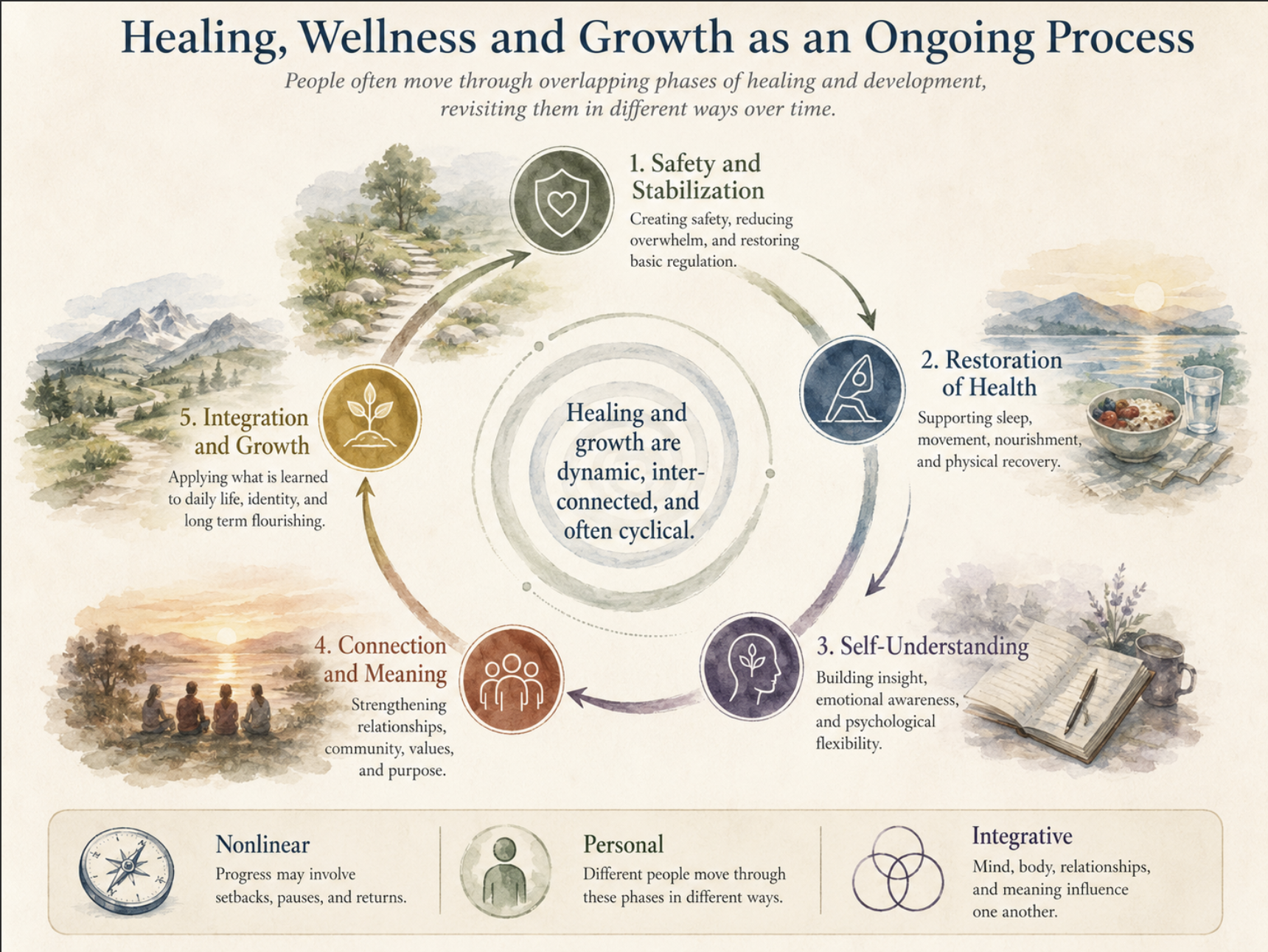
Figure 4. Healing, Wellness and Growth as an Ongoing Process.
Pathway categories and how they differ
A useful taxonomy distinguishes pathways by the kind of change they are designed to support. Some reduce symptoms, some restore functioning, some build skills, some support identity or meaning, some create community, and some offer education or experience.
This taxonomy also protects against overgeneralization. Therapists, coaches, retreat facilitators, meditation teachers, breathwork guides, sound practitioners, course creators, product vendors, attorneys, and business service providers may all belong in the broader ecosystem, but they do not serve the same function.
This is also why the Atlas should be built as a branching reference system rather than a collection of isolated promotional pages. The foundational article defines the whole landscape. Branch articles explain categories. More specific articles can then connect readers to providers, products, courses, legal resources, and educational materials without confusing discovery with medical advice or unsupported promises.
For Psychedelist, these distinctions matter structurally. Therapy, coaching, retreats, meditation, somatic work, sound experiences, courses, products, and legal resources should each have their own category logic, evidence language, risk language, and user expectations.
Spiritual and meaning-centered pathways address questions of purpose, identity, values, mortality, forgiveness, suffering, transcendence, and belonging to something larger than the individual self. These pathways may involve religion, Indigenous traditions, contemplative practice, philosophy, service, nature, ritual, or personal reflection. They should be described with care because spiritual language can be profound for some readers and inappropriate or alienating for others. A mature Atlas can acknowledge meaning and spirituality as major dimensions of human life while still distinguishing them from clinical treatment, commercial promises, and unsupported certainty [93].
Community pathways emphasize belonging, witnessing, shared practice, and social support. Human beings are not isolated self-improvement projects. Relationships can regulate emotion, buffer stress, reinforce habits, provide practical help, and give meaning to growth. Community can also harm when it becomes coercive, exclusionary, shaming, or dependent on a charismatic authority. A professional framework must therefore recognize both the health importance of connection and the need for boundaries, transparency, and personal agency [94].
Experiential pathways work through direct experience. Retreats, contemplative practice, somatic work, expressive arts, movement, ritual, nature exposure, and sound-based practices may create insight or regulation, but integration into daily life determines much of their long-term value.
Educational pathways focus on knowledge, skills, and understanding. A person may learn about trauma, communication, mindfulness, nutrition, exercise, sleep, neuroscience, meaning, spiritual traditions, legal issues, or professional practice. Education can change behavior by giving people language for what they are experiencing and practical tools for what to do next. At the same time, information alone is often insufficient. Many people need relationships, structure, repetition, accountability, practice, and supportive environments before knowledge becomes embodied change [96].
Nonclinical support pathways serve a different function. Coaching, mentorship, education, peer support, meditation instruction, breathwork classes, sound-based experiences, nature-based programs, and many retreats may support reflection, learning, habit formation, community, emotional regulation, or personal growth. They should not be represented as substitutes for medical or mental health care when a person needs clinical assessment or treatment. Their value often depends on fit, facilitator skill, setting, boundaries, group culture, preparation, and integration rather than a single therapeutic mechanism [97].
A central purpose of the Atlas is to distinguish different kinds of pathways without forcing them into one category. Clinical pathways are designed to assess, diagnose, treat, or manage defined health conditions. They may include psychotherapy, medical care, psychiatry, ketamine treatment, physical rehabilitation, nutrition care, or other licensed health services. These pathways require special attention to training, licensure, informed consent, documentation, contraindications, and emergency procedures. Their claims should be measured against clinical evidence and professional standards [98].
Ethics, safety and responsible guidance
Any article about healing and growth must address ethics and safety. People seeking healing are often vulnerable. They may be grieving, traumatized, depressed, isolated, physically ill, spiritually searching, or desperate for relief. This creates responsibility for educators, providers, platforms, retreat centers, coaches, clinicians, and advertisers.
Ethical guidance begins with scope. Clinicians, coaches, spiritual teachers, facilitators, bodyworkers, nutrition professionals, and retreat leaders have different responsibilities. Problems arise when a provider presents themselves as qualified beyond their training, licensure, or role.
Safety also includes screening. Certain practices may be inappropriate for some individuals because of medical conditions, psychiatric history, pregnancy, cardiovascular risk, trauma history, medications, substance use, or legal status. Psychedelic-assisted therapies, intensive breathwork, fasting, extreme exercise, deep somatic release, and prolonged meditation retreats can all carry risks. Responsible providers do not promise universal benefit. They screen, inform, refer, document, and provide follow-up.
Evidence transparency is another ethical requirement. Some pathways are supported by strong meta-analytic evidence for specific outcomes. Others are supported by preliminary studies, traditional use, theory, clinical experience, or personal testimony. These categories should not be blurred. A high-quality learning center can respect tradition and lived experience while still distinguishing them from peer-reviewed evidence.
Finally, ethical healing requires attention to power. Helpers can influence belief, identity, sexuality, money, spirituality, medical decisions, and social belonging. Strong boundaries, consent, cultural humility, privacy, and accountability are essential. Professionalism is not only about citations. It is about protecting the reader and participant from inflated claims, coercion, dependency, and harm.
Research limits and future directions
The evidence base for healing, wellness, and growth is broad but uneven. Some areas, such as physical activity, sleep duration, social relationships, cognitive behavioral therapy, nutrition patterns, and chronic disease prevention, have extensive research foundations [99]. Other areas, such as certain somatic therapies, integrative care models, complex retreat settings, and psychedelic-assisted therapies, are promising but require more research, clearer standards, and longer follow-up [100].
Whole person research is difficult because it asks questions that do not fit neatly into single-variable models. Many interventions are multicomponent. Many outcomes are multisystem. Human beings change over time. Social context matters. Treatment effects differ across individuals. The NCCIH workshop summary on methodological approaches for whole person research highlights the need for methods that can study interconnected systems, multicomponent interventions, and multisystem outcomes [101].
Complex adaptive systems thinking also changes research expectations. Not every important outcome can be captured by a single randomized trial. Randomized trials are powerful for many questions, but observational data, qualitative research, longitudinal cohorts, mixed-methods designs, comparative effectiveness research, and systems modeling may also be needed [102]. The goal is not to lower standards. The goal is to use appropriate standards for complex questions.
Future research should also measure broader outcomes. VanderWeele argued that empirical studies often focus on narrow outcomes and should more often examine flourishing broadly, including health, happiness, meaning, character, relationships, and stability [103]. This is especially relevant for healing and growth pathways. A meditation program might reduce stress but also influence meaning. A retreat might increase connection but also require integration. A nutrition intervention might improve metabolic markers and mood. A therapy might reduce symptoms and improve relationships.
The future of this field will likely involve integration across medicine, psychology, neuroscience, public health, social science, contemplative studies, environmental health, and ethical technology. The strongest learning center articles will not merely summarize isolated practices. They will help readers understand how multiple sources of evidence fit into a coherent map of human flourishing.
Practical evaluation of providers and pathways
Readers evaluating a provider, retreat, coach, therapist, clinic, or wellness program can use a simple professional framework. First, identify the primary goal. Is the person seeking symptom relief, trauma recovery, physical health, relationship repair, spiritual growth, self-understanding, community, or education? Second, identify the pathway category. Is the service clinical, educational, experiential, spiritual, body-based, lifestyle-based, nature-based, or medical? Third, identify the evidence level and risks. What is known? What is uncertain? What screening is required?
Fourth, evaluate credentials and scope. Does the provider have training appropriate to the claim? Are they licensed where licensure is required? Do they describe limits? Do they refer out when necessary? Fifth, evaluate consent and safety. Are risks explained? Are participants pressured? Is confidentiality respected? Are emergency procedures in place? Sixth, evaluate integration. What happens after the session, retreat, or program? How does the experience become part of daily life?
This evaluation framework can be applied across the Psychedelist ecosystem. A therapy listing should be evaluated differently from a coaching listing. A retreat should be evaluated differently from a nutrition provider. A psychedelic-assisted service should be evaluated with special attention to legality, screening, medical oversight, preparation, support, and integration. A meditation program should clarify intensity and suitability. A body-based practice should clarify touch, consent, contraindications, and trauma sensitivity.
The purpose is not to make readers suspicious of every provider. It is to help them become informed participants. Good providers should welcome informed questions. They should be able to explain what they do, who it is for, what evidence supports it, what risks exist, what they do not treat, and how they protect participants. That transparency builds trust and distinguishes professional care from hype.
For the Learning Center, this practical layer is where encyclopedia-quality education becomes useful to the reader. The article explains the map. Provider pages and category pages can then help readers navigate the territory with better judgment.
Conclusion
Healing, wellness, and growth pathways are best understood as interconnected routes through which people seek relief, vitality, meaning, connection, resilience, and flourishing. The evidence does not support a single path for all people. It supports a multi-domain framework grounded in physical health, mental health, relationships, environment, meaning, education, community, and whole person systems.
The most credible foundation begins with what is broadly supported: sleep, movement, nutrition, psychological care, social connection, purpose, supportive environments, and public health. More specialized pathways, including integrative medicine, somatic approaches, retreats, contemplative practices, and psychedelic-assisted therapies, may contribute for selected individuals and goals when used responsibly. Their value depends on evidence, safety, context, practitioner competence, and integration.
Human flourishing is not a final state that can be purchased, prescribed, or reached once and for all. It is an ongoing process of becoming healthier, more connected, more capable, more purposeful, and more responsive to life. It involves the body, mind, relationships, environment, behavior, beliefs, experience, and meaning. It is personal, but not isolated. It is individual, but also social. It is biological, but also psychological, relational, cultural, and existential.
A professional learning center should therefore offer more than inspiration. It should offer orientation. It should help readers understand the major pathways, compare them responsibly, recognize risks, and make informed decisions. At its best, such a resource becomes a map of the human journey: many goals, many pathways, one interconnected living system.
See also
Treatment and Support Pathways for Healing, Wellness and Growth
Coaching, Mentorship and Personal Growth
Retreats and Immersive Experiences
Psychedelic-Assisted Support, Preparation and Integration
Somatic and Body-Based Approaches
Nature, Environment and Healing
Human Flourishing and Whole Person Health
How to Evaluate Healing and Wellness Providers
References
Citations
The numbered citations below correspond to the bracketed reference numbers used in the article. A single citation note may cite one or several works; the Sources section lists the full bibliography.
1. WHO mental health 2025; WHO social determinants report 2025; Borrell-Carrio et al. 2004; WHO health promotion 2009; NCCIH strategic plan 2021; VanderWeele 2017.
2. NCCIH strategic plan 2021; Plsek and Greenhalgh 2001; NCCIH whole person research workshop 2021; VanderWeele 2017.
3. VanderWeele 2017.
4. WHO physical activity guidelines 2020; Warburton et al. 2006; Watson et al. 2015; DGAC 2020; Katz and Meller 2014; WHO chronic disease report 2005; Mitchell et al. 2021; Wilkinson et al. 2018; Luoma et al. 2020; de Vos et al. 2021; Griffiths et al. 2008; Nour et al. 2016.
5. WHO health promotion 2009.
6. WHO social determinants report 2025; Solar and Irwin 2010; WHO mental health determinants 2014.
7. Mateos-Aparicio and Rodriguez-Moreno 2019.
8. Hofmann et al. 2012; Hayes et al. 2006; Kashdan and Rottenberg 2010.
9. VanderWeele 2017.
10. WHO mental health 2025.
11. WHO social determinants report 2025; Solar and Irwin 2010.
12. Borrell-Carrio et al. 2004.
13. VanderWeele 2017.
14. Ryff 2014.
15. Ryan and Deci 2000.
16. Seligman 2018; Bolier et al. 2013; Park et al. 2004.
17. Steger 2017.
18. NCCIH strategic plan 2021; NCCIH whole person research workshop 2021.
19. NCCIH strategic plan 2021; NCCIH whole person research workshop 2021.
20. Plsek and Greenhalgh 2001.
21. van Klaveren et al. 2019; PMI Working Group 2015; Kent et al. 2018.
22. van Klaveren et al. 2019; Kent et al. 2018.
23. WHO physical activity guidelines 2020; Warburton et al. 2006; Watson et al. 2015; DGAC 2020; Katz and Meller 2014; WHO chronic disease report 2005.
24. WHO physical activity guidelines 2020; Warburton et al. 2006; Pedersen and Saltin 2015.
25. Watson et al. 2015.
26. DGAC 2020; Katz and Meller 2014.
27. WHO chronic disease report 2005.
28. Mateos-Aparicio and Rodriguez-Moreno 2019.
29. Hofmann et al. 2012; Hayes et al. 2006; Kashdan and Rottenberg 2010; Grossman et al. 2004; Goyal et al. 2014.
30. WHO mental health 2025; Ryff 2014; Ryan and Deci 2000.
31. Hofmann et al. 2012.
32. Hayes et al. 2006.
33. Kashdan and Rottenberg 2010.
34. Southwick et al. 2014.
35. Hofmann et al. 2012; Hayes et al. 2006.
36. Kashdan and Rottenberg 2010.
37. Holt-Lunstad et al. 2010; Holt-Lunstad et al. 2015; WHO mental health determinants 2014; Coan and Maresh 2014.
38. Russo et al. 2017; Joseph et al. 2005; Rohricht 2009.
39. Holt-Lunstad et al. 2010; Holt-Lunstad et al. 2015.
40. WHO mental health determinants 2014.
41. Coan and Maresh 2014.
42. Lee and Kim 2015.
43. WHO social determinants report 2025; Solar and Irwin 2010; Srinivasan et al. 2003.
44. Twohig-Bennett and Jones 2018.
45. Capaldi et al. 2014.
46. Kaplan 1995.
47. Ulrich 1983.
48. Kellert 1997.
49. Srinivasan et al. 2003.
50. Hill and Turiano 2014; Frankl 1992; Steger 2017; VanderWeele 2017.
51. Frankl 1992.
52. Hill and Turiano 2014.
53. VanderWeele 2017.
54. Steger 2017.
55. Seligman 2018.
56. VanderWeele 2017.
57. Bolier et al. 2013.
58. Park et al. 2004.
59. Csikszentmihalyi 2014.
60. Grossman et al. 2004.
61. Goyal et al. 2014.
62. Hayes et al. 2006; Kashdan and Rottenberg 2010.
63. Russo et al. 2017; Joseph et al. 2005.
64. Rohricht 2009.
65. Porges 2011.
66. IOM integrative medicine summit 2009.
67. Maizes et al. 2009.
68. Epstein and Street 2011.
69. Mead and Bower 2000.
70. Jonas et al. 2013.
71. Vickers et al. 2012.
72. WHO physical activity guidelines 2020; Warburton et al. 2006; Watson et al. 2015; DGAC 2020; Katz and Meller 2014; WHO chronic disease report 2005; Pedersen and Saltin 2015.
73. Katz and Meller 2014.
74. DGAC 2020.
75. Pedersen and Saltin 2015.
76. WHO social determinants report 2025; Solar and Irwin 2010.
77. VanderWeele 2017.
78. Plsek and Greenhalgh 2001; NCCIH whole person research workshop 2021.
79. Mitchell et al. 2021; Wilkinson et al. 2018; Luoma et al. 2020; de Vos et al. 2021; Griffiths et al. 2008; Nour et al. 2016.
80. Mitchell et al. 2021.
81. Wilkinson et al. 2018.
82. Luoma et al. 2020.
83. de Vos et al. 2021.
84. Griffiths et al. 2008.
85. Nour et al. 2016.
86. Frankl 1992.
87. Grossman et al. 2004; Goyal et al. 2014.
88. Griffiths et al. 2008; Nour et al. 2016.
89. Seligman 2018; Bolier et al. 2013; Park et al. 2004; Steger 2017; VanderWeele 2017.
90. Hofmann et al. 2012.
91. Hayes et al. 2006.
92. Ryff 2014; Ryan and Deci 2000; Southwick et al. 2014; Hofmann et al. 2012; Hayes et al. 2006; Kashdan and Rottenberg 2010; Twohig-Bennett and Jones 2018; Capaldi et al. 2014; Hill and Turiano 2014; Frankl 1992; Csikszentmihalyi 2014; Steger 2017.
93. VanderWeele 2017; Frankl 1992; Steger 2017.
94. Holt-Lunstad et al. 2010; Holt-Lunstad et al. 2015; Coan and Maresh 2014.
95. Twohig-Bennett and Jones 2018; Grossman et al. 2004; Mitchell et al. 2021; Luoma et al. 2020.
96. Ryan and Deci 2000; Hayes et al. 2006; Kashdan and Rottenberg 2010.
97. Ryan and Deci 2000; Southwick et al. 2014; Bolier et al. 2013.
98. Hofmann et al. 2012; Maizes et al. 2009; Epstein and Street 2011.
99. WHO physical activity guidelines 2020; Warburton et al. 2006; Watson et al. 2015; DGAC 2020; Katz and Meller 2014; WHO chronic disease report 2005; Hofmann et al. 2012; Holt-Lunstad et al. 2010; Holt-Lunstad et al. 2015.
100. Rohricht 2009; Mitchell et al. 2021; Wilkinson et al. 2018; Luoma et al. 2020; de Vos et al. 2021; Griffiths et al. 2008; Nour et al. 2016; Jonas et al. 2013.
101. NCCIH whole person research workshop 2021.
102. Plsek and Greenhalgh 2001; NCCIH whole person research workshop 2021.
103. VanderWeele 2017.
Sources
1. World Health Organization. (2025). Mental health. (Source page)
2. Mateos-Aparicio, P., & Rodriguez-Moreno, A. (2019). The impact of studying brain plasticity. Frontiers in Cellular Neuroscience, 13, Article 66. (Source page)
3. World Health Organization. (2025). World report on social determinants of health equity. (Source page)
4. Borrell-Carrio, F., Suchman, A. L., & Epstein, R. M. (2004). The biopsychosocial model 25 years later: Principles, practice, and scientific inquiry. Annals of Family Medicine, 2(6), 576-582. (Source page)
5. World Health Organization. (2009). Milestones in Health Promotion: Statements from Global Conferences. Geneva: World Health Organization. Ottawa Charter for Health Promotion, pp. 1-5. (Source page)
6. National Center for Complementary and Integrative Health. (2021). NCCIH Strategic Plan FY 2021-2025: Mapping a Pathway to Research on Whole Person Health. Bethesda, MD: U.S. Department of Health and Human Services, National Institutes of Health. (Source page)
7. Institute of Medicine. (2009). Integrative Medicine and the Health of the Public: A Summary of the February 2009 Summit. Washington, DC: The National Academies Press. (Source page)
8. VanderWeele, T. J. (2017). On the promotion of human flourishing. Proceedings of the National Academy of Sciences, 114(31), 8148-8156. (Source page)
9. van Klaveren, D., Balan, T. A., Steyerberg, E. W., & Kent, D. M. (2019). Models with interactions overestimated heterogeneity of treatment effects and were prone to treatment mistargeting. Journal of Clinical Epidemiology, 114, 72-83. (Source page)
10. Precision Medicine Initiative Working Group. (2015). The Precision Medicine Initiative Cohort Program: Building a Research Foundation for 21st Century Medicine. Report to the Advisory Committee to the Director, National Institutes of Health. (Source page)
11. Kent, D. M., Steyerberg, E. W., & van Klaveren, D. (2018). Personalized evidence based medicine: Predictive approaches to heterogeneous treatment effects. BMJ, 363, k4245. (Source page)
12. Solar, O., & Irwin, A. (2010). A Conceptual Framework for Action on the Social Determinants of Health. Geneva: World Health Organization. Social Determinants of Health Discussion Paper 2. (Source page)
13. World Health Organization. (2020). WHO Guidelines on Physical Activity and Sedentary Behaviour. Geneva: World Health Organization. (Source page)
14. Warburton, D. E. R., Nicol, C. W., & Bredin, S. S. D. (2006). Health benefits of physical activity: The evidence. CMAJ, 174(6), 801-809. (Source page)
15. Watson, N. F., et al. (2015). Joint Consensus Statement of the American Academy of Sleep Medicine and Sleep Research Society on the Recommended Amount of Sleep for a Healthy Adult: Methodology and Discussion. Journal of Clinical Sleep Medicine, 11(8), 931-952. (Source page)
16. Dietary Guidelines Advisory Committee. (2020). Scientific Report of the 2020 Dietary Guidelines Advisory Committee. Advisory Report to the Secretary of Agriculture and Secretary of Health and Human Services. (Source page)
17. Katz, D. L., & Meller, S. (2014). Can we say what diet is best for health? Annual Review of Public Health, 35, 83-103. (Source page)
18. World Health Organization. (2005). Preventing Chronic Diseases: A Vital Investment. Geneva: World Health Organization. (Source page)
19. Ryff, C. D. (2014). Psychological well-being revisited: Advances in science and practice. Psychotherapy and Psychosomatics, 83(1), 10-28. (Source page)
20. Ryan, R. M., & Deci, E. L. (2000). Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. American Psychologist, 55(1), 68-78. (Source page)
21. Southwick, S. M., Bonanno, G. A., Masten, A. S., Panter-Brick, C., & Yehuda, R. (2014). Resilience definitions, theory, and challenges: Interdisciplinary perspectives. European Journal of Psychotraumatology, 5, 25338. (Source page)
22. Hofmann, S. G., Asnaani, A., Vonk, I. J. J., Sawyer, A. T., & Fang, A. (2012). The efficacy of cognitive behavioral therapy: A review of meta-analyses. Cognitive Therapy and Research, 36(5), 427-440. (Source page)
23. Hayes, S. C., Luoma, J. B., Bond, F. W., Masuda, A., & Lillis, J. (2006). Acceptance and Commitment Therapy: Model, processes and outcomes. Behaviour Research and Therapy, 44(1), 1-25. (Source page)
24. Kashdan, T. B., & Rottenberg, J. (2010). Psychological flexibility as a fundamental aspect of health. Clinical Psychology Review, 30(7), 865-878. (Source page)
25. Holt-Lunstad, J., Smith, T. B., & Layton, J. B. (2010). Social relationships and mortality risk: A meta-analytic review. PLoS Medicine, 7(7), e1000316. (Source page)
26. Holt-Lunstad, J., Smith, T. B., Baker, M., Harris, T., & Stephenson, D. (2015). Loneliness and social isolation as risk factors for mortality: A meta-analytic review. Perspectives on Psychological Science, 10(2), 227-237. (Source page)
27. World Health Organization & Calouste Gulbenkian Foundation. (2014). Social Determinants of Mental Health. Geneva: World Health Organization. (Source page)
28. Lee, S. J., & Kim, Y. (2015). Searching for the meaning of community well-being. In S. J. Lee, Y. Kim, & R. Phillips (Eds.), Community Well-Being and Community Development: Conceptions and Applications (pp. 9-23). Springer International Publishing. (Source page)
29. Coan, J. A., & Maresh, E. L. (2014). Social baseline theory and the social regulation of emotion. In J. J. Gross (Ed.), Handbook of Emotion Regulation (2nd ed., pp. 221-236). Guilford Press. (Source page)
30. Twohig-Bennett, C., & Jones, A. (2018). The health benefits of the great outdoors: A systematic review and meta-analysis of greenspace exposure and health outcomes. Environmental Research, 166, 628-637. (Source page)
31. Capaldi, C. A., Dopko, R. L., & Zelenski, J. M. (2014). The relationship between nature connectedness and happiness: A meta-analysis. Frontiers in Psychology, 5, Article 976. (Source page)
32. Kaplan, S. (1995). The restorative benefits of nature: Toward an integrative framework. Journal of Environmental Psychology, 15(3), 169-182. (Source page)
33. Ulrich, R. S. (1983). Aesthetic and affective response to natural environment. In I. Altman & J. Wohlwill (Eds.), Human Behavior and Environment, Vol. 6: Behavior and the Natural Environment (pp. 85-125). Plenum Press. (Source page)
34. Srinivasan, S., O'Fallon, L. R., & Dearry, A. (2003). Creating healthy communities, healthy homes, healthy people: Initiating a research agenda on the built environment and public health. American Journal of Public Health, 93(9), 1446-1450. (Source page)
35. Kellert, S. R. (1997). The biophilia hypothesis: Aristotelian echoes of the good life. In S. R. Kellert & E. O. Wilson (Eds.), The Biophilia Hypothesis (pp. 140-172). Island Press. (Source page)
36. Hill, P. L., & Turiano, N. A. (2014). Purpose in life as a predictor of mortality across adulthood. Psychological Science, 25(7), 1482-1486. (Source page)
37. Las Heras, M., Grau-Grau, M., & Rofcanin, Y. (Eds.). (2023). Human Flourishing: A Multidisciplinary Perspective on Neuroscience, Health, Organizations and Arts. Springer Nature. (Source page)
38. Frankl, V. E. (1992). Man's Search for Meaning: An Introduction to Logotherapy (4th ed.). Beacon Press. Original work published 1946. (Source page)
39. Grossman, P., Niemann, L., Schmidt, S., & Walach, H. (2004). Mindfulness-based stress reduction and health benefits: A meta-analysis. Journal of Psychosomatic Research, 57(1), 35-43. (Source page)
40. Csikszentmihalyi, M. (2014). Flow and the Foundations of Positive Psychology. Springer. (Source page)
41. Seligman, M. E. P. (2018). PERMA and the building blocks of well-being. The Journal of Positive Psychology, 13(4), 333-335. (Source page)
42. Goyal, M., et al. (2014). Meditation programs for psychological stress and well-being: A systematic review and meta-analysis. JAMA Internal Medicine, 174(3), 357-368. (Source page)
43. Russo, M. A., Santarelli, D. M., & O'Rourke, D. (2017). The physiological effects of slow breathing in the healthy human. Breathe, 13(4), 298-309. (Source page)
44. Joseph, C. N., Porta, C., Casucci, G., Casiraghi, N., Maffeis, M., Rossi, M., & Bernardi, L. (2005). Slow breathing improves arterial baroreflex sensitivity and decreases blood pressure in essential hypertension. Hypertension, 46(4), 714-718. (Source page)
45. Rohricht, F. (2009). Body oriented psychotherapy. The state of the art in empirical research and evidence-based practice: A clinical perspective. Body, Movement and Dance in Psychotherapy, 4(2), 135-156. (Source page)
46. Porges, S. W. (2011). The Polyvagal Theory: Neurophysiological Foundations of Emotions, Attachment, Communication, and Self-Regulation. W. W. Norton & Company. (Source page)
47. Vickers, A. J., et al. (2012). Acupuncture for chronic pain: Individual patient data meta-analysis. Archives of Internal Medicine, 172(19), 1444-1453. (Source page)
48. Maizes, V., Rakel, D., & Niemiec, C. (2009). Integrative Medicine and Patient-Centered Care. Commissioned paper for the Institute of Medicine Summit on Integrative Medicine and the Health of the Public. Washington, DC: Institute of Medicine. (Source page)
49. Epstein, R. M., & Street, R. L., Jr. (2011). The values and value of patient-centered care. Annals of Family Medicine, 9(2), 100-103. (Source page)
50. Mead, N., & Bower, P. (2000). Patient-centredness: A conceptual framework and review of the empirical literature. Social Science & Medicine, 51(7), 1087-1110. (Source page)
51. Pedersen, B. K., & Saltin, B. (2015). Exercise as medicine - evidence for prescribing exercise as therapy in 26 different chronic diseases. Scandinavian Journal of Medicine & Science in Sports, 25(Suppl. 3), 1-72. (Source page)
52. Bolier, L., Haverman, M., Westerhof, G. J., Riper, H., Smit, F., & Bohlmeijer, E. (2013). Positive psychology interventions: A meta-analysis of randomized controlled studies. BMC Public Health, 13, 119. (Source page)
53. Park, N., Peterson, C., & Seligman, M. E. P. (2004). Strengths of character and well-being. Journal of Social and Clinical Psychology, 23(5), 603-619. (Source page)
54. Steger, M. F. (2017). Meaning in life and wellbeing. In M. Slade, L. Oades, & A. Jarden (Eds.), Wellbeing, Recovery and Mental Health (pp. 75-85). Cambridge University Press. (Source page)
55. Mitchell, J. M., et al. (2021). MDMA-assisted therapy for severe PTSD: A randomized, double-blind, placebo-controlled phase 3 study. Nature Medicine, 27(6), 1025-1033. (Source page)
56. Wilkinson, S. T., et al. (2018). The effect of a single dose of intravenous ketamine on suicidal ideation: A systematic review and individual participant data meta-analysis. American Journal of Psychiatry, 175(2), 150-158. (Source page)
57. Luoma, J. B., Chwyl, C., Bathje, G. J., Davis, A. K., & Lancelotta, R. (2020). A meta-analysis of placebo-controlled trials of psychedelic-assisted therapy. Journal of Psychoactive Drugs, 52(4), 289-299. (Source page)
58. de Vos, C. M. H., Mason, N. L., & Kuypers, K. P. C. (2021). Psychedelics and neuroplasticity: A systematic review unraveling the biological underpinnings of psychedelics. Frontiers in Psychiatry, 12, 724606. (Source page)
59. Griffiths, R. R., Richards, W. A., Johnson, M. W., McCann, U. D., & Jesse, R. (2008). Mystical-type experiences occasioned by psilocybin mediate the attribution of personal meaning and spiritual significance 14 months later. Journal of Psychopharmacology, 22(6), 621-632. (Source page)
60. Nour, M. M., Evans, L., Nutt, D., & Carhart-Harris, R. L. (2016). Ego-dissolution and psychedelics: Validation of the Ego-Dissolution Inventory (EDI). Frontiers in Human Neuroscience, 10, 269. (Source page)
61. Plsek, P. E., & Greenhalgh, T. (2001). The challenge of complexity in health care. BMJ, 323(7313), 625-628. (Source page)
62. Jonas, W. B., Eisenberg, D., Hufford, D., & Crawford, C. (2013). The evolution of complementary and alternative medicine (CAM) in the USA over the last 20 years. Forschende Komplementarmedizin, 20(1), 65-72. (Source page)
63. National Center for Complementary and Integrative Health. (2021). Methodological Approaches for Whole Person Research Workshop Summary. National Institutes of Health. Bethesda, MD: NCCIH. (Source page)